Mesenteric Lymphadenitis:
Causes, Symptoms, Diagnosis and Treatment
Mesenteric lymphadenitis is a common cause of right-sided abdominal pain in children, that mimics appendicitis. Though more common in children, it can occur in adults too. We will discuss the causes, how to diagnose it and the best treatment options available for this condition.

It is estimated that up to 20 percent of children who are diagnosed with acute appendicitis actually do not have appendicitis, but acute mesenteric lymphadenitis - also called non-specific mesenteric adenitis.
Mesenteric lymphadenitis is the inflammation of the lymph nodes on the wall of the mesentery (the covering of the intestines) in the absence of appendicitis, leading to abdominal pain.
In some children, there will be associated nausea, vomiting and fever.
Typically, the child with mesenteric adenitis will look well, or just mildly unwell, yet with complaints of abdominal pain.
What Causes Mesenteric Lymphadenitis?
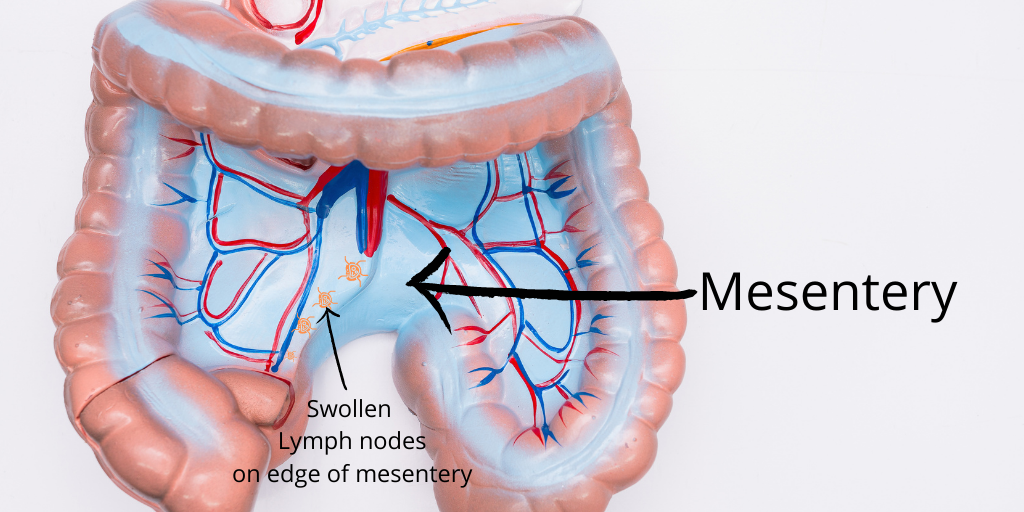
Our intestines are clasped and hung in place by a sheet of thick membrane like a free-flowing towel called the mesentery. This allows the intestines to be free to move as well as fixed to the floor of back of our abdomen.
The mesentery contains arteries, veins and lymph nodes.
Like lymph nodes elsewhere in the body, they swell to produce and recruit white blood cells to fight off invading bacteria, fungi or virus if we catch an infection. You almost certainly must have had one of such swollen lymph nodes or glands in your neck sometime in the past when you had a very bad cold.
When lymph nodes along the edge of the mesentery of your child swells in response to an infection, it can cause abdominal pain. This is what is referred to as mesenteric lymphadenitis (inflammation of the lymph nodes along the mesentery).
The following are the usual causes of mesenteric lymphadenitis:
Viruses
Several studies have shown that up to 60 percent of mesenteric lymphadenitis are caused by viruses. The common cold viruses are the most implicated, including:
- Adenoviruses
- Non-SARS coronaviruses,
- Coxsackie A and B viruses
- Epstein-Barr virus
- HIV virus.
Bacteria
Bacteria contamination of food can mesenteric lymphadenitis. The following are the often implicated bacteria causing mesenteric adenitis. They include:
- Yersinia enterocolitica (found in improperly cooked pork, beef, lamb, fish, and oyster and reported by the Centre for Disease Control (CD) as the cause of over 115,000 illnesses and 600 hospitalizations every year in the USA alone
- Streptococcus viridans
- Salmonella
- Bartonella henselae
- Yersinia pseudotuberculosis
- Campylobacter jejuni.
While Streptococcus viridans, Campylobacter and Pseudo tuberculosis infection are common world wide, infection by Yersinia enterocolitica is mostly found in the cold regions of the world, especially in Europe and America.
Parasitic Protozoa
Parasitic protozoa has also been shown to cause mesenteric adenitis. These include:
- Giardia lamblia
- Toxoplasma gondii
- Cryptosporidium infection (cryptosporidiosis)
Any of these infections - virus, bacteria or parasite can get into our intestine and get trapped inside the lymph nodes on the mesentery and trigger and inflammation, leading to the enlargement of the lymph nodes and the symptoms of mesenteric lymphadenitis.
What Are The Symptoms of Mesenteric Lymphadenitis?
Mesenteric adenitis is more common in the first 10 years of life, especially before the 6th birthday. It affects boys and girls equally, although Yersinia-linked infections are seen more in boys.
The signs and symptoms of mesenteric lymphadenitis are very similar to those of appendicitis, except for some subtle differences.
They include :
Abdominal Pain
Is mesenteric lymphadenitis painful? Yes. Abdominal pain is the most frequent symptom of mesenteric lymphadenitis. The following are the characteristics of the pain in lymphadenitis of the mesentery.
- The pain typically starts in the upper abdomen just above the umbilicus
- The child will point to a vague area around the umbilicus when asked where did the pain start from
- It then moves to the right lower abdominal quadrant
- The pain could be just a mild pain or severe
- Some kids will experience intermittent bouts of colicky pain that resolves momentarily without any intervention, becoming completely pain-free between attacks
- The pain will get better after a day or two while in acute appendicitis, the pain would worsen with each passing day and your child would look more unwell
- The pain moves from one spot to the other within the abdomen, in keeping with the movement of the bowel loops within the abdominal cavity. Klein's sign of shifting tenderness, also known as Alder's sign can be demonstrated - if the child were to lay on the left side for a few minutes and then re-examined, the point of tenderness on his or her abdomen moves from the right to the left of the original spot.
- In appendicitis, the pain may initially start around the umbilicus, then moves over to the right iliac fossa. Once it settles there, it does not move around any longer.
Preceding Cold or Sore Throat
One symptom that gives away the diagnosis of mesenteric lymphadenitis is that of the presence of cold or sore throat in the days or week before the onset of abdominal pain.
There may even still be an on going cough and cold in the child. The neck glands, if examined may be swollen.
Fever
About half of children with mesenteric lymphadenitis would have associated fever.
The degree of fever may vary from very mild - 37.5 to 39, but averages 38 degrees Celsius.
Vomiting
A few patients with mesenteric lymphadenitis will vomit. Those who vomit tend to do so very early in the course of their illness and around when they start complaining of pain in the abdomen.
Appendicitis is most unlikely if a child vomits before onset of abdominal pain. This is usually a late symptom in acute appendicitis.
Diarrhoea
Diarrhoea is one of the not very frequent but possible symptoms your child could have if suffering with mesenteric lymphadenitis. This is even more so in the case of Yersinia induced infection. Recent pork ingestion is also a pointer to possible Yersinia infection as the culprit.
Children with acute appendicitis can also suffer with diarrhoea, but this is often a later symptom and the diarrhoea in acute appendicitis is usually mild.
Anorexia
More often than not, with mesenteric lymphadenitis, your child would still be able to eat and drink. Appetite is more likely to be preserved. If a your child complains of abdominal pain and his or her appetite remains good, it is mesenteric lymphadenitis. In acute appendicitis, appetite is lost pretty quickly and in most cases.
How Is Mesenteric Lymphadenitis Diagnosed?
Nothing is more distressing than to see your child suffering with pain in the abdomen and doctors trying to make up their mind if this is a case of acute appendicitis that requires an immediate operation or if this is a case of acute mesenteric lymphadenitis that does not require a surgical operation.
The main aim of the doctor is to establish that this is indeed an adenitis of the mesenteric lymph glands and not a more serious condition like:
- Acute appendicitis
- Crohn's disease
- Acute ileitis
- Intussusception
- Ruptured or twisted right ovarian cyst
- Diabetic ketoacidosis
- Urinary tract infection
- Constipation
- Ectopic pregnancy
Or indeed any other condition that mimics acute non-specific mesenteric lymphadenitis that may require surgery or other form of specific intervention. You can see a list of conditions that mimics mesenteric lymphadenitis here.
To make a firm diagnosis of acute mesenteric lymphadenitis, at least all the following 3 conditions must be met:
- The child would present with a new onset pain in his or her right lower abdomen
- A CT scan of the abdomen will show a normal appendix (that is, an appendix that is not inflamed in anyway)
- The Ct scan would also show a few swollen lymph nodes in the intestinal mesentery. Any lymph node 5 to 8 mm in size or even more meets this criteria.

{kind=link}
In other to arrive at this findings, the following tests need to be done:
Full Blood Count (Complete Blood Count)
This is a simple quick blood test routinely done for many conditions. Also called complete blood count, it is a test that shows the amount and quality of the components of blood itself - the amount of red blood cells, white blood cells, platelets, and percentage of plasma.
In most cases of acute inflammation or infection, the white blood cell (WBC) count will be raised, particularly the subtypes called the neutrophils and sometimes the lymphocytes.
This test will not tell us much except that there is evidence of infection. In the first day or two, there will be increase in white blood cells (leucocytosis) which settles on the third day, while in acute appendicitis, the white blood cell count increases with every day of infection until the diseased appendix is removed or treated with antibiotics.
Yersinia Enterocolitica Serology
This is also a blood test.
Where there is a history of recent pork consumption or if you live in an area where there is an outbreak of Yersinia infection, a Yersinia serology may be necessary to make a diagnosis of Yersinia enterocolitica mesenteric adenitis.
This is even more so if your child has diarrhea as well as right lower abdominal pain, anorexia and fever.
Urine Test (Urinalysis)
This is a test to check the urine of your child to be sure that his or her symptoms are not due to a urinary tract infection - infection involving the bladder or kidneys.
Your child will be required to pass urine sample which is tested for the presence or absence of blood, leucocytes and nitrates as well as ketones and sugar.
Acute DKA or diabetic ketoacidosis can mimic mesenteric lymphadenitis in children as well as acute appendicitis and UTI.
Abdominal Ultrasound Scan
This is often the first preferred investigation in children, since it is non –invasive, and there is no exposure to radiation (X-rays).
It may help demonstrate small pebble shaped and sized hypo-echoic 5 to 8 mm nodules, which will be quite different from the surrounding tissues. Thickening of the mesentery will also support a diagnosis of mesenteric adenitis.
As well as the presence of these swollen lymph nodes, the appendix will show normal signs with no evidence of inflammation to make a diagnosis of acute mesenteric lymphadenitis.
Computed Tomography (CT) Scan
With the huge improvement in CT scan technology, providing better resolution with lesser amount of radiation exposure, as well as its increased available in many countries, a CT scan is almost routine now in the investigation of abdominal pain.
A new onset pain in the right lower abdomen is certainly an indication for the use of CT scan. This will help increase the chances of a definite diagnosis and avoid an unnecessary surgical operation.
In acute mesenteric lymphadenitis, a CT scan with both oral and intravenous contrast is necessary.
A contrast CT will demonstrate enlarged mesenteric lymph nodes. The contrast helps to differentiate the lymph nodes from blood vessels better than when a contrast or dye is not used. CT scan is better able to measure the lymph nodes to be greater than 5 mm in size to be classified as enlarged, in the mesentery.
This plus a normal appendix helps in the confirmation of this condition.
Barium Enema
A barium enema is rarely necessary in the workup for the diagnosis of mesenteric lymphadenitis. It is nevertheless an option available in countries where access the CT scan is limited.
Barium enema done for lymphadenitis of the mesentery may show indentation of the bowel walls from pressure by the enlarged mesenteric lymph nodes.
Laparoscopy
If the diagnosis is still in doubt, a laparoscopy may lay it to rest.
At laparoscopy, the lymph nodes surrounding the terminal ileum and colon may be found to be more in number and enlarged, with swelling of the mesentery, and a normal looking appendix.
One or two enlarged lymph nodes could be harvested and cultured as well as examined under the microscope (histology) to determine the exact cause of the lymphadenitis is desired.
How Do You Treat Mesenteric Lymphadenitis?
Mesenteric lymphadenitis is usually a benign illness, which will get better on its own without treatment.
Once the diagnosis is confirmed, the approach to treatment will depend on what is suspected to be the exact cause of the lymphadenitis.
The following are the treatment options for acute mesenteric lymphadenitis depending on what the presumed or confirmed cause is:
Virus
If your child had cold symptoms followed by complaints of pain in his or her right lower abdomen, then the most likely cause is virus. As stated above, cold viruses are the most frequent causes of acute non-specific mesenteric lymphadenitis.
In such a case, treatment will be mainly symptomatic or supportive. Treatment will include:
- Tylenol (Paracetamol) or Ibuprofen (Advil®, MOTRIN®) given every 6 to 8 hourly to help with pain and fever.
- Encourage drinking clear fluids to keep hydrated
- Rest
- Regular observation to ensure that condition does not deteriorate.
Yersinia
If you live in an area where Yersinia infection outbreak is declared or common or if there your child had eaten pork in the past few days, then Yersinia infection is likely.
The best treatment option for Yersinia infection involve the use of the following antibiotics:
- Fluoroquinolones like ciprofloxacin, norfloxacin, olfloxacin or levofloxacin either alone or in combination. Studies have shown this group of antibiotics to be most effective treatment for Yersinia infection.
- Trimethoprim-Sulfamethoxazole - commonly sold as Septrin or Sulfa in many countries. This is another very effective choice of antibiotics in the treatment of Yersinia enterocolitica mesenteric adenitis.
- Cephalosporins. The 3rd generation cephalosporins like Cefixime, Cefotaxime and ceftriaxone have been documented to be great choice against this organism.
Protozoa
Protozoa induced mesenteric adenitis can be treated with the appropriate anti-protozoan medication.
- Toxoplasmosis gondii infection is treated with Sulfadiazine or Pyrimethamine
- Cryptosporidium infection is treated with Nitazoxanide or Azithromycin
- Giardia lamblia is treated with Metronidazole.
A few cases of mesenteric lymphadenitis could be serious and a broad spectrum antibiotics as well as intravenous fluid administration may be necessary or even outright surgical operation to remove a section of diseased bowel plus the appendix.
Is Mesenteric Lymphadenitis Serious?
Is mesenteric lymphadenitis serious? This is a commonly asked question. The short answer is no. It is not serious usually.
Most children who develop this condition will get well without any intervention in a few days or up to 4 weeks. However, in a few cases, it could led to serious infection needing treatment as stated above.
ICD 10 Dx Code for Mesenteric Lymphadenitis
The ICD10 diagnostic code for mesenteric lymphadenitis or adenitis is 188.0 and the ICD 9 CM code for this condition is 289.2.

|
||
| search engine by freefind |
Sign Up For
Our Newsletter
Recent Articles
-
Anxiety stomach Pains caused by possible cancer return
Jul 06, 23 02:54 PM
Diagnosed with Prostate Cancer 16 years ago. Over the last 2 years my PSA results have started to climb, therefore yesterday I had a full body bone scan -
Left upper Quadrant pain for 18 months!
Mar 27, 22 06:55 PM
Hi, About 18 months ago I had to call an ambulance as I had severe pain in my abdomen on the left side. I was discharged and they told me it was an intercostal -
Mesenteric Lymphadenitis - Causes, Symptoms, Diagnosis and Treatment
Sep 19, 20 04:16 PM
 Mesenteric lymphadenitis is a common cause of right-sided abdominal pain in children, that mimics appendicitis. Though more common in children, it can occur in
Mesenteric lymphadenitis is a common cause of right-sided abdominal pain in children, that mimics appendicitis. Though more common in children, it can occur in


Disclaimer : The information provided on this website is for educational purposes only. It is not a substitute for seeking a one-to-one professional medical advice and treatment.
ALWAYS consult your doctor or healthcare provider to see if the information provided here applies to your personal situation and for personalized care.
The presence of hyperlinks from this website to external organizations does not constitute an approval, recommendation or endorsement of these organizations. They are provided for convenience only.
ABDOPAIN.com and its affiliates disclaim any and all warranty or liability for the use or lack of use of any and all information on this website. If you have a medical emergency, call your local emergency medical service.