|
Cholecystitis
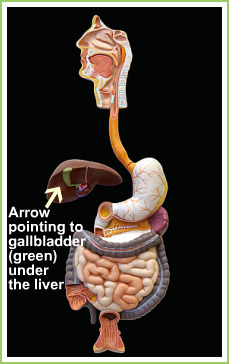
Cholecystitis is the medical word used to describe inflammation of the gall bladder. The gallbladder is a pear shaped sac lying just under the liver.It is where bile is stored. It is usually caused by obstruction of the exit duct of the gallbladder. There may be no stone involved (acalculus). Sometimes a semi-solid stone still in formation called sludge is the culprit. Even though for the most times bacterial infection is associated with disease, it is believed that the infection is a consequence and not the cause of the disease. This makes sense as it is usually the stone or sludge that causes irritation before the bugs get in. As explained in the section on gallbladder diseases, gallstones are formed when bile, which is produced in the liver and stored in the gallbladder, looses so much water and becomes very concentrated that it super saturates. Crystals are then formed. These crystals aggregate to form gallstones. The stones may be silent, causing no problem or symptoms. Over time, the stones may multiply in number or grow in size or both and cause continuous irritation to gallbladder. The gallbladder then become inflamed, the same as your skin could become sore from continuous scratches and banging by a rough stone. Bugs then get into this inflammatory soup formed. This disease is more common in the fair, fat, fertile, female, of forty or fifty-something years old, of northern European origin. Having said that, any body, from any age and race can suffer from this disease. Patients with sickle-cell disease are also prone to gallstones and thus Cholecystitis from repeated haemolysis, forming lots of pigment stones from the break down products of red blood. About half a million persons in the United States alone develop Cholecystitis yearly. Cholecystitis if complicated can lead to death. In fact, if the gallbladder ruptures following untreated Cholecystitis, as high as 60% ( 6 out of 10 persons) of patients die later in the hospital. HOW DO I KNOW I HAVE CHOLECYSTITIS Cholecystitis usually presents as pain high up in the abdomen, above the umbilicus (belly button), or to the right upper abdomen. The pain is usually continuous and may spread to the right side of the chest, over to the back, under the wing bone. Pain may be severe, but dull and boring. Pain may be worsened by eating fatty meals. There may be associated nausea and vomiting. The vomiting may be very bitter; containing loads of bile. There may be feverishness. This pain could last for several hours to days, unlike in Biliary colic that last for only a couple of hours. Placing your hands under the right breast and gently pushing may reveal some tenderness. A few patients may develop yellowish coloration in the white of the eye called jaundice. TESTS TO CONFIRM CHOLECYSTITIS There are quite a few tests you could be required to carry out. First, if you think you have Cholecystitis, the wise thing to do is to contact your G.P. There are now G.Ps you could speak to 27 hours of the day via confidential telephone calls or online. On of such G.P services is the 24/7 GP There are also private laboratories regulated by the government that can arrange to have investigations done for you from home or work place as needed, and your result sent to your G.P for interpretation and treatment if need be. Now, you may be required to have some blood tests, abdominal and chest x-rays, as well as an ultrasound scan. BLOOD TESTS The blood tests you will be required to do may include Full blood count (FBC), Electrolyte and urea (U/E or DAX or), Liver function test (LFT), Cryo-reactive proteins (CRP), Amylase level and Arterial Blood Gas in very severe cases. None of these tests are specific for Cholecystitis. A blood culture may be necessary if temperature is very high. In Cholecystitis, because there is usually the involvement of some kind of bugs, the body would recruit white blood cells from their storage points in the body to fight these bugs. This will cause an elevation in the WBC (white blood cell) count, which is a component of the FBC. Normal level is any where in the region of 4,000 – 11,000 (2,800 – 8, 5000 in blacks). The U/E may be normal. Often, the liver function test LFT may show elevated ALT and AST as well as elevated bilirubin level. CRP may be moderately raised. Amylase is usually normal, except there are other conditions that cause elevation like Pancreatitis, perforated peptic ulcer, or dead gut (Ischaemic colitis) all which can present like Cholecystitis. Again, normal blood picture does not mean you may not have Cholecystitis, neither does a deranged result confirms you have the disease. It may only mean there is an increased likelihood you have Cholecystitis. The whole picture is usually put together by the attending physician in conjunction with other investigations findings and experience. ABDOMINAL X-RAY There are at least two reasons why an abdominal X-ray may be requested. First, since 80 to 90% of gallstones are cholesterol stones, some 10 to 20% of stones (pigment stones containing calcium salts) will show up on X-ray. Secondly, the cause of your abdominal pain may not be due to Cholecystitis. Something else could show up on the X-ray. CHEST X-RAY Lower lobe pneumonia or some heart problems could present like Cholecystitis. Even pancreatitis, or perforated peptic ulcer can be confused with Cholecystitis. A chest x-ray may show gas under the diaphragm in perforated peptic ulcer. ULTRASOUND SCAN This is the best diagnostic test for gallstones. It picks up 90 – 95% of stones or sludge in the gall bladder. It is readily available, devoid of radiation, and non-invasive.In some centres, CT-Scan is also required. This could provide more information about the gallbladder, especially with its relationship with other structures. However, CT scan is not the investigation of choice in uncomplicated Cholecystitis. It is much more expensive, and exposes one to an enormous amount of radiation. TREATMENT OPTIONS Once the diagnosis of Cholecystitis is made, the decision to treat follows.In the accident and emergency department, the immediate prerogative would be to control patient’s pain, replace fluid loss from vomiting and fever, and identify / prevent further complications where possible. Antibiotics are used where evidence of infection exists. Patient may be asked to refrain from eating or drinking in the first 12 – 24 hours to rest the gallbladder, as well as a precautionary measure, should the need for an emergency operational intervention arises (e.g. if the gallbladder is found to be perforated!). Once the inflammation has settled, the patient can commence sips of clear fluids and graduate to eating a low fat or even fat free diet. In very ill patients not responding to treatment, there may be need for percutaneous drainage (drainage through the skin) of the gallbladder under radiological control, as a means of controlling infection, especially when such patient is unfit for surgery due to a pre-existing medical condition like heart or lungs disease. After the first 48 hours, definitive treatment options are often then taken.The treatment options available include: • Surgery • Medical treatment • Lithotripsy • Endoscopic Retrograde Cholangio-Pancreatography (ERCP) It is basically a cameral test. The endoscope is a long flexible tube, about the size of a pen. At its end is a cameral and good light source. It may have attached to it a videoscope or fibreoptic light system that transmits images to a screen. This is combined with the use of X – ray and dye. After giving a sedative, the doctor introduces the endoscope through the mouth down to the upper small intestine (Duodenum)Read More on ERCP
If you choose to, you can help keep this site free by making very little donations. Some have donated £0.20. We will only provide you with relevant links, and no unnecessary advertising. Your sponsorship will cover the cost of running this site and of writing the information herein.
|
[?]Subscribe To This Site
|



